
Ewing Sarcoma
General Information
What is it?
Aggressive, high-metastasis risk bone sarcoma and malignancy of mesenchymal progenitor cells most commonly in long bones (e.g., femur, tibia), but also pelvis, axial skeleton, and more
- Also known as an Askin tumor, extraosseous sarcoma
Risk Factors: chromosomal translocations (EWS-FLI-1 formation, EWS-ERG fusion), younger individuals (10-15 yrs; rare >40 yrs)
Evaluation
- Symptoms: intermittent pain worsening at night/during sleep, swelling, stiffness
- If metastasized: systemic (weight loss, fever), respiratory symptoms/pleural signs
- Imaging: MRI/CT, radiographs (“moth” lesions, “Codman triangle”)
- Confirming EWS-FLI1 fusion: In situ hybridization (FISH), RT-PCR for amplification
- Open biopsy
- Histological pearls (see below)
Types
- Localized: limited to the area of origination
- Metastatic: spread past local lymph nodes to other organs
- Recurrent: recurring malignancy after initially treated
Pathophysiology
- Chromosomal translocations, gene rearrangements
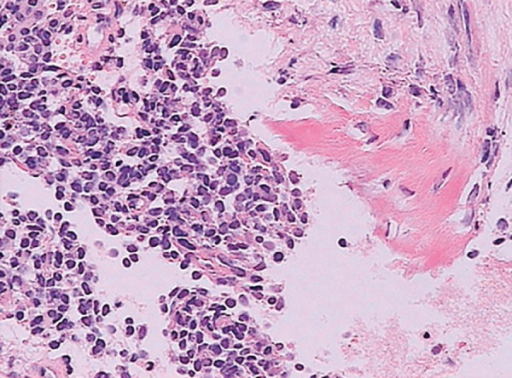
Histological Characteristics
Small, poorly differentiated round cells with round nuclei, stippled/fine chromatin
Pseudorosettes (around central eosinophilic staining) or perivascular patterns with necrotic/”dark” cells
Decreased cytoplasmic-nuclear ratio with abundant glycogen (PAS-positive, diatase degradable), scant clear cytoplasm
+CD99, MIC2 expression: facilitates migration of leukocytes to the endothelium
Other biomarkers: vimentin, CD45, synaptophysin, chromogranin

Treatment
Systemic therapies
- VDC with alternating IE: vincristine/doxorubicin/cyclophosphamide
Surgery (limb sparing, amputation), radiotherapy (preoperative, definitive, adjuvant)
Stem cell transplants

Leave a comment