
Melanoma
General Information
What is it?
Most aggressive (highest risk of metastasis) carcinoma, originating from melanocytes
Risk Factors: UV exposure (e.g. tanning beds), genetic predisposition, childhood sunburns, light hair/iris color, high freckly density, multiple melanocytic nevi/moles
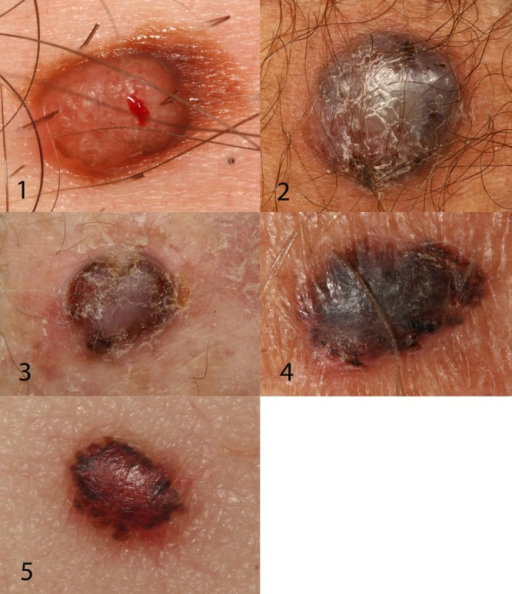
Clinical Diagnosis: pigmented lesions, often bleeds or ulcerates (dependent on subtype); can see secondary lesions in eyes due to melanocyte origin; neuro crest cell origination, thus can manifest in related cells
ABCDE method for examining lesions:
- Asymmetry
- Borders are uneven
- Color is dark or uneven
- Diameter >6mm
- Evolving characteristics (shape, size, color)
Pathophysiology:
- BRAF V600E mutation: activates MAP pathway which induces cellular proliferation
Major Subtypes
Superficial Spreading
Most common subtype
Pigmented macule/papule with irregular border and asymmetry
No dermal invasion, radial growth

Nodular
Second most common but more aggressive than SF melanoma
Palpable, pigmented lesion (or can be amelanotic) on sun exposed areas
Vertical growth phase (no radial growth) with limited epidermal spread
Acral Lentiginous
Most common in people of African or Asian descent
Typically found in palms, soles, under nails (subungual manifestation, presents as longitudinal dark band): Hutchinson’s sign – involvement of proximal nail fold (see below)
Unevenly pigmented


Lentigo Maligna
Lesions on face, scalp, neck; in older individuals
Begins as lentigo-like macule, develops into larger and darker foci
When confined to epidermis, presents as nonpalpable macule

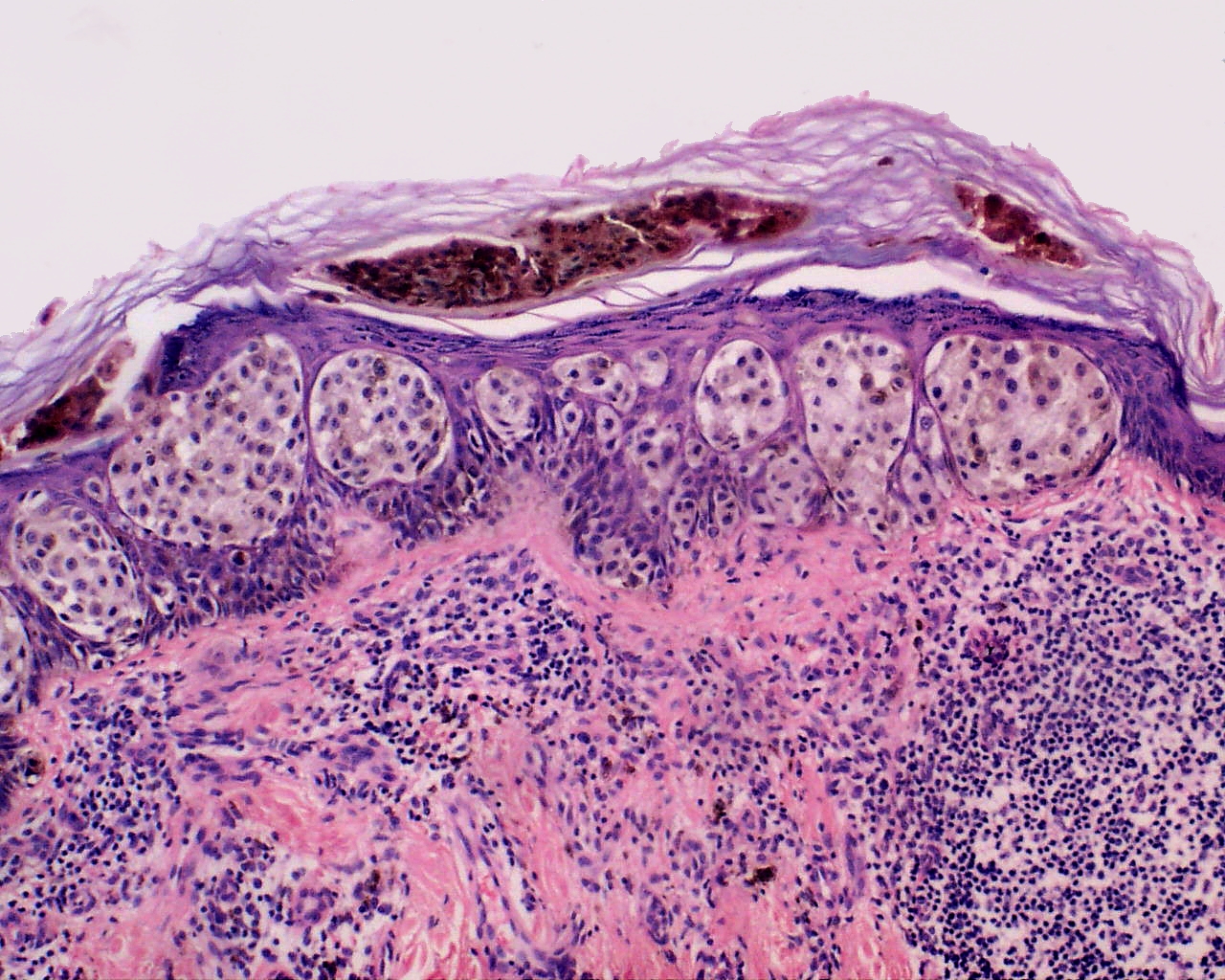
Histological Characteristics
Malignant cellular growth at dermal epidermal junction
See nests of melanocytes
Types of growth
- Pagetoid spread: basal malignancy moves towards upper epidermal layers
- Confluent growth: increased proportion of melanocytes, replace normal basal keratinocytes
Unzipping artifact: damage to hemidesmosomes leads to separation of epidermis and dermis visible on histo (due to blister like lesion), evidence of confluent growth
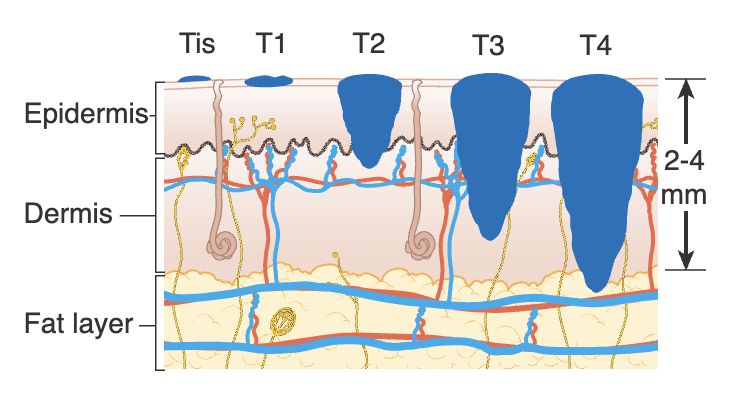
Stages
& corresponding surgical intervention
0. S0 (in situ) limited to epidermis; wide excision to muscle fascia
1. SI <2mm, N0, M0; wide excision down to muscle fascia, sentinel lymph node biopsy (SNLB)
2. SII >1mm, N0, M0; Keytruda immune checkpoint inhibitor; radiation therapy, if SNLB positive is S3
3. SIII local lymph node metastasis, M0; LN dissection and wide excision; Keytruda, radiation therapy
4. SIV distant metastasis; palliative care

Leave a comment