
Psoriasis
General Information
What is it?
Autoimmune disease of skin, nails, and joints that most commonly presents with well-demarcated silvery scales and plaques (especially over extensor surfaces, scalp, lumbarsacral region)
Risk Factors: genetic (PSOR1 on CHR6, HLA-Cw6), infections (Streptococcus), hypocalcemia, drugs (antimalarials, beta blockers, lithium), systemic steroid withdrawal, women, seasonal (aggravated in winter)
Evaluation
- Symptoms: plaques, pustules, erythema, pain, pruritus
- Lab biomarkers:
- Rheumatoid factor: negative
- CBC, comprehensive metabolic panel for renal/liver function tests
- Elevated ESR, uric acid
Types
- Type I: positive family history, <40 yr, associated with HLA-Cw6
- Type 2: no family history, >40 yr, no HLA association
- Subtypes (see below)
Pathophysiology
- Helper T cell (Th1) activation, releasing inflammatory agents (TNFα, IFy, interleukins)
- Proinflammatory molecules stimulate keratinocyte proliferation, forming plaques
- Erythema stimulated from overexpression of antimicrobial peptides
- Little oil/sebum production results in scales
Major Subtypes
Plaque
Most common subtype (85-90% of patients)
Erythematous plaques along extensor surfaces (elbows, knees, scalp) that often worsen in winter
Symmetrical (bilateral) distribution
Auspitz sign: bleeding points upon removal of scales

Guttate (Eruptive)
Common secondary to upper respiratory tract infection (primarily Strep)
Most common in adolescents or young adults
Small, scattered erythematous, raindrop-shaped lesions over the trunk and back

Pustular
Erythematous pus-filled lesions (pustules)
Can be localized (small patches) vs generalized/von Zumbusch (sterile pustules across the entire body; associated with hypocalcemia)
Often presents acutely with leukocytosis, fever, malaise
RFs: pregnancy, withdrawal from glucocorticoids

Erythrodermic
Widespread inflammation (>90% body) with pain, pruritus, and swelling
Desquamative scales
Due to exacerbation of unstable plaque psoriasis and withdrawal from systemic steroids, leading to sepsis or insensible perspiration

Subtypes (cont.)
Inverse (flexural/intertriginous): sharply demarcated patches along skin folds (groins, armpits, intergluteal)
- Presents without scales
Sebopsoriasis: red plaques with greasy scales along thin skin (with sebaceous glands
Nail manifestations (see here): pitting, leukonychia, oil drop signs
Other signs
- Koebner phenomenon: new papules at the site of previous trauma
- Woronoff ring: blanching area around resolving plaques
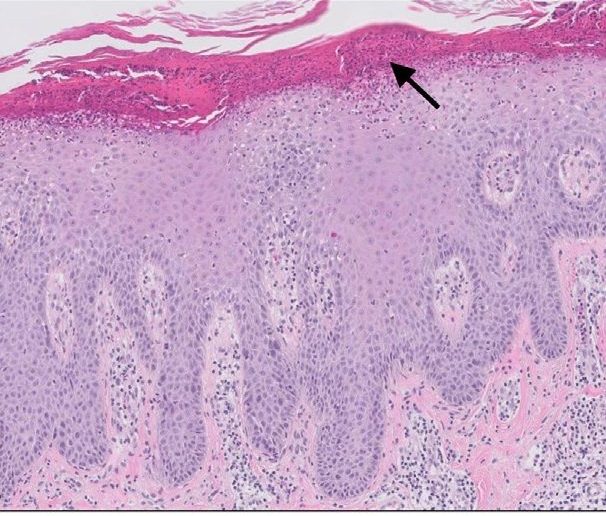
Histological Characteristics
Acanthosis
Parakeratosis with neutrophil aggregation
Alternating hypogranulosis and hypergranulosis
Absence of granular lesions
Dilated and tortuous capillaries in the dermis
Treatment
Topical
- Corticosteroids, Vitamin D analogs, coal tar
- Emollients and moisturizer for barrier function
Systemic: methotrexate, cyclosporine (especially with nail involvement)
Biologic: TNF inhibitors, IL12/17/23 inhibitors
Light therapy: UVB, PUVA (311-313 nm)

Leave a comment