
Rosacea
General Information
What is it?
Chronic autoimmune inflammatory disease that is differentiable from true acne or acne vulgaris; is also colloquially known as “adult acne”
Most commonly affects forehead, nose/mid cheeks, chin and often manifests symmetrically/bilaterally
Risk Factors: genetic predisposition, demodex mites, Heliobacter pylori, UV rays, medication, celtic heritage
Evaluation:
Signs & Symptoms (see below regarding specific subtypes)
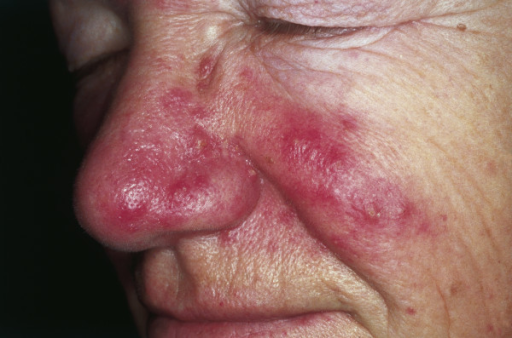
- Central facial erythema and redness (Figure 1)
- Pustules/papules
- Telangiectasias: visible veins and vasculature (seen more often in older individuals)
- Rhinophyma
- Eye/ocular involvement
Pathophysiology
Autoimmune activation of immune system
- Overexpression of Th1/Th17 and TLR-2 (associated with increased activity of mast cells)
Increased expression of matrix metalloproteinases and VEGF
Lymphatic vasodilation, increasing release of vasoactive peptides
Demodex mite infestation or H.pylori infection
Clinical Subtypes
Note that patients may present with multiple subtypes, and have evolving symptomatology.
Erythemato-telangiectactic
Persistent erythema and flushing (central facial region)
The most common subtype and clinical manifestation
Papulopustuler, “Adult Acne”
Presents similarly to acne vulgaris due to eruption of papules and pustules (but unlike acne, individuals with rosacea do not have comedones

Phymatous
Presents with nose enlargement (rhinophyma)
- Can also affect the chin (mentophyma), forehead (metophyma), ears (otophyma), eyelids (bleherophyma)
- Pathophysiology
- Hypertrophic sebaceous glands, sebum plugging
- Fluid leakage into dermis leading to inflammation and fibrosis
Typically in older males
Is due to more developed, untreated, chronic rosacea
Ocular
Presents with dryness, redness, blurred vision, light sensitivity
Also blepharitis (eyelid inflammation), conjunctivitis (pink eye), keratitis (corneal inflammation), iritis (iris inflammation), lid margin telangiectasia
Treatment
Lifestyle modifications
Avoid triggering factors, minimize UV exposure (SPF), gentle moisturizers and skincare products
By subtype symptomatology
Erythema: brimonidine tartrate gel, oxymetazoline HCL gel
Inflammation: topical cyclines, metronidazole (avoid retinal)
Demodex mites: ivermectin
Rhinophyma: doxyxycline, isotretinoin, tetracycline
- If surgical removal (if permanently enlarged): must be off isotretinoin
- Reduce hypertrophy of sebaceous glands, recontour nasal region
- Excisional treatment
- Graft reconstruction
- Cryosurgery
- Laser surgery

Leave a comment